
INDICATIONS for HEMODYNAMIC MONITORING
Hypovolemic shock
Cardiogenic shock
Hypovolemic shock
- Due to a reduction in circulating blood volume resulting from either hemorrhage or fluid depletion.
- Preload is markedly decreased, leading to inadequate ventricular filling.
- The patient with hypovolemic shock manifests hypotension and tachycardia.
- Systemic, venous, and intracardiac pressures are abnormally low.
- The overall PAC pressure tracing has a damped appearance.
- Is the most common cause of death in intensive care units in the United States, most often caused by sepsis.
- Septic shock is an example of distributive shock, a form of shock characterized by profound peripheral vasodilation.
- Although the CO may be normal or even elevated in this type of shock, organ and tissue perfusion are inadequate.
- Swan-Ganz catheter measurements frequently demonstrate low filling pressures.
Cardiogenic shock
- Cardiogenic shock is the result of severe depression in cardiac performance.
- It is often caused by LV pump failure caused by acute myocardial infarction or severe mitral or aortic valve disease
- Cardiogenic shock is characterized by systolic blood pressure less than 80 mm Hg, cardiac index less than 1.8 L/min/m2, and PCWP greater than 18 mm Hg.
- This form of shock can occur from a direct insult to the myocardium ( large acute MI, severe cardiomyopathy) or from a mechanical problem that overwhelms the functional capacity of the myocardium (acute severe mitral regurgitation, acute ventricular septal defect)
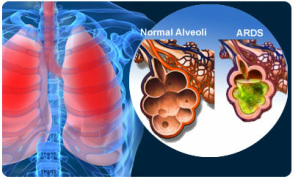
ARDS ( Acute Respiratory Distress Syndrome) ~ ARDS starts with acute lung injury (ALI), which kills about 75,000 Americans a year and whose risk increases with age. ~ ARDS itself develops from an injury to the alveoli, the site of gas exchange.
~ The goal of care for ARDS patients is to maximize perfusion in the pulmonary capillary system by increasing oxygen transport between the alveoli and pulmonary capillaries.
~ To achieve the goal, you need to increase fluid volume without overloading the patient. This is done by careful hemodynamic monitoring.
~ The goal of care for ARDS patients is to maximize perfusion in the pulmonary capillary system by increasing oxygen transport between the alveoli and pulmonary capillaries.
~ To achieve the goal, you need to increase fluid volume without overloading the patient. This is done by careful hemodynamic monitoring.
