The study of hemodynamics has its own vocabulary and requires an understanding of the interactions between the heart, blood vessels, and blood.
The cardiac output pushes the blood through the vascular system.
~ Cardiac output (CO) is calculated by multiplying the heart rate (HR) by the stroke volume (SV).
~ Cardiac output/cardiac index are used to assess the heart’s ability to meet the body’s oxygen demands.
~ Cardiac index is a more precise measurement of heart function since body size affects overall cardiac output.
~The cardiac index is a calculation of cardiac output per square meter of body surface area.
The normal cardiac index is 2.8-4.2 L/min/m2.
CO = SV x HR.
Normal resting CO is 4-8 L/min and varies with body size.
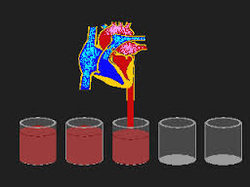
Stroke volume is the volume of blood pumped out of the heart with each heartbeat. If the stroke volume drops, the body will compensate by increasing the heart rate to maintain cardiac output. This is known as compensatory tachycardia. Tachycardia is an effective compensatory mechanism up to a point. At heart rates greater than 150 bpm, diastolic filling time becomes so short that the tachycardia itself produces a drop in stroke volume, and cardiac output can no longer be maintained. Stroke volume is affected by three factors, preload, afterload, and contractility.
The cardiac output pushes the blood through the vascular system.
~ Cardiac output (CO) is calculated by multiplying the heart rate (HR) by the stroke volume (SV).
~ Cardiac output/cardiac index are used to assess the heart’s ability to meet the body’s oxygen demands.
~ Cardiac index is a more precise measurement of heart function since body size affects overall cardiac output.
~The cardiac index is a calculation of cardiac output per square meter of body surface area.
The normal cardiac index is 2.8-4.2 L/min/m2.
CO = SV x HR.
Normal resting CO is 4-8 L/min and varies with body size.
Stroke volume is the volume of blood pumped out of the heart with each heartbeat. If the stroke volume drops, the body will compensate by increasing the heart rate to maintain cardiac output. This is known as compensatory tachycardia. Tachycardia is an effective compensatory mechanism up to a point. At heart rates greater than 150 bpm, diastolic filling time becomes so short that the tachycardia itself produces a drop in stroke volume, and cardiac output can no longer be maintained. Stroke volume is affected by three factors, preload, afterload, and contractility.
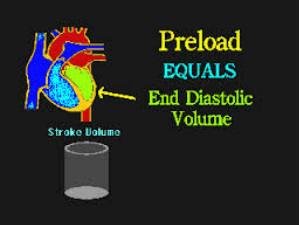
Preload is the force that stretches the muscle fibers of a resting heart – how much they are stretched just prior to contraction. It is the degree of muscle fiber stretching present in the ventricles right before systole
- Is the amount of blood in a ventricle before it contracts; also known as “filling pressures”.
- The amount of blood present within the right and left atria and ventricles prior to contraction and the condition of the myocardium determine the stretch or preload of the heart muscle.
- The greater the volume of blood in a heart chamber, the greater the preload.
- Ideally, an adequately filled and stretched left ventricle should briskly contract, snap like a rubber band, to send blood on its way
- Left ventricular preload is reflected by the PCWP
- Right ventricular preload is reflected by the CVP (RA).
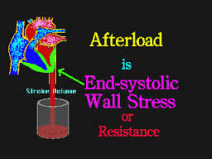
Afterload is defined as the resistance that the ventricle must overcome to eject its volume of blood.
- Any resistance against which the ventricles must pump in order to eject its volume
- How hard the heart [either side left or right] has to push to get the blood out
- Also thought of as the “ resistance to flow” or how “clamped” the blood vessels are
- As arterial vessels constrict, the afterload increases; as they dilate, afterload decreases.
- High afterload increases myocardial work and decreases stroke volume.
- Low afterload decreases myocardial work and results in increased stroke volume.
- As preload (fluid volume) increases, cardiac output will also increase until the cardiac output levels off.
- Too little preload and the cardiac output cannot propel enough blood forward, too much and the
- heart will become overwhelmed leading to failure.
- Just the right amount of preload produces the best possible cardiac output; finding this level of preload is called “preload optimization.”

Contractility when used in a discussion of hemodynamics, the term contractility refers to the inherent ability of the cardiac muscle to contract regardless of preload or afterload status.
